This guideline has now been superseeded by the 2015 intubation guidelines click here
Difficult Airway Society 2007
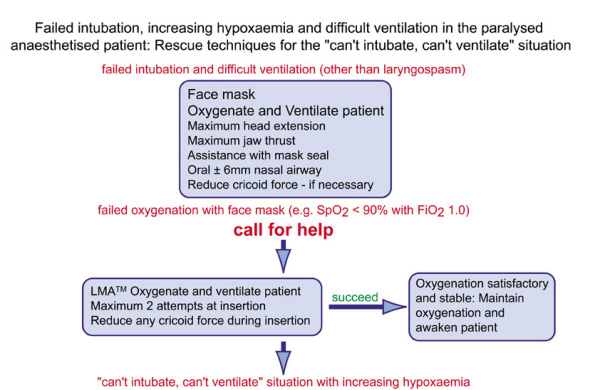
The scenario is of a patient under general anaesthesia with muscle relaxation who cannot be intubated by direct laryngoscopy and in whom mask ventilation is difficult/impossible.
Notes:
- Do not waste time trying to intubate when oxygenation is the priority.
- Consider whether laryngospasm is the problem (treat this initially with further IV anaesthesia increments).
- A large oral airway and four hands holding the facemask/applying jaw thrust and neck extension with another person squeezing the bag might be defined as optimal facemask inflation. If it fails go onto the next step.
- Place a classic laryngeal mask. An excellent, life-saving device. Some suggest that it is more sensible to place this than struggle with difficult facemask ventilation. If it fails to provide an airway leave it in situ, to provide route for egress of air if needle cricothyrotomy needed.
- It is possible that, if suxamethonium is used, its rapid offset will allow the patient to 'wake-up' and regain their own airway before serious hypoxia ensues. However, there is no guarantee of this.
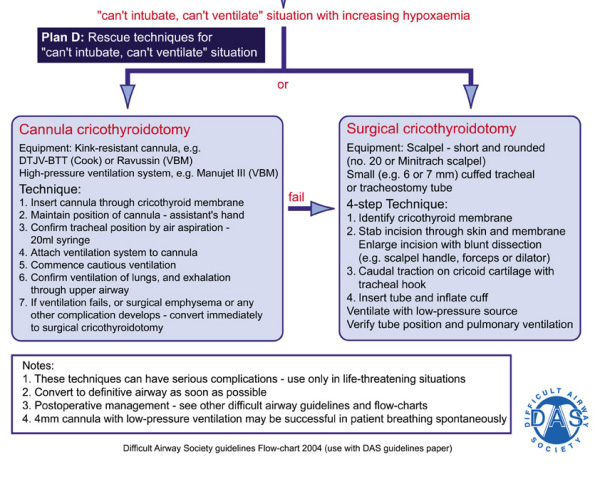
- With failed intubation, failed facemask and failed laryngeal mask ventilation (CVCI can't-ventilate-can't-intubate, or CICO can't-intubate-can't-oxygenate) carry on now to emergency cricothyrotomy to provide emergency oxygenation with prepared kit.
Areas for discussion
Emergency cricothyrotomy is one of the mannikin/skills room core skills. Each anaesthetist should know which kit is used in the hospital, where it is located in the anaesthetic room and how to use it. It is one of the items to address in an induction period.
Purpose built cannulae with a diameter exceeding 4 mm (up to 6 mm for cricothyrotomy) are available. Some are cannula over needle and some are Seldinger method kits. Cuffed and cuffless kits are available (e.g. Melker). They allow use of the normal breathing system, allow attachment of capnography and avoid barotrauma. However, there is little evidence that a 4 mm uncuffed tube can resuscitate an adult patient unless the upper airway is completely occluded to expiration. It is this lack of evidence-base which has meant that cricothyrotomy with a purpose-built cannula of 4-6 mm does not appear on the 2004 guidelines.
Emergency cricothyrotomy by any technique is uncommon in theatre-based anaesthesia care (more common in trauma). DAS would be delighted to hear of any attempts at emergency cricothyrotomy in earnest, noting what kit was used and whether it was successful. Please send details to [email protected]
